einstein (São Paulo). 11/Mar/2026;24(spe2):eAO1805.
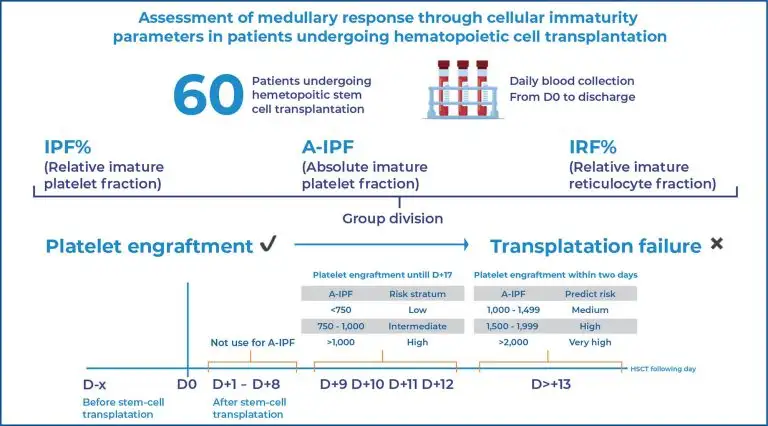
Assessment of medullary response through cellular immaturity parameters in patients undergoing hematopoietic stem cell transplantation
DOI: 10.31744/einstein_journal/2026AO1805
Highlights
■ A-IPF can be used as a biomarker for platelet engraftment after hematopoietic stem cell transplantation.
■ IPF% and IRF% are not reliable biomarkers for bone marrow engraftment after hematopoietic stem cell transplantation.
■ IPF%, A-IPF, and IRF% do not support safe reduction of prophylactic platelet transfusions.
■ Cellular immaturity parameters lack standardized quality control measures for harmonization between clinical and research laboratories.
ABSTRACT
Objective:
This study aimed to evaluate relative immature platelet fraction (IPF%), absolute immature platelet fraction (A-IPF), and relative immature reticulocyte fraction (IRF%) as biomarkers of bone marrow recovery after hematopoietic stem cell transplantation and to assess their potential role in reducing prophylactic platelet transfusions.
Methods:
Sixty hematopoietic stem cell transplantation recipients (mean age, 50 years) were analyzed, and sex-specific reference ranges for IPF%, A-IPF, and IRF% were established. The predictive performance for platelet engraftment and transfusion requirements was assessed using receiver operating characteristic curve analysis, logistic regression, Fine-Gray competing risks models, Cox regression, and negative binomial modeling.
Results:
Only A-IPF differed significantly between groups. An A-IPF threshold greater than 1,450 predicted platelet engraftments within two days with a sensitivity of 82.1% and a specificity of 80.0%. Logistic regression demonstrated a 2.3-fold increase in the likelihood of platelet engraftment for every 1,000-unit increase in A-IPF, and Fine-Gray analysis confirmed a higher cumulative incidence of engraftment in the intermediate and high A-IPF strata (subdistribution hazard ratios, 2.71 and 3.58; p<0.001). All patients required platelet transfusions (149 events). Cox regression identified A-IPF as an independent risk factor for transfusion (hazard ratio, 1.0001; p=0.027), whereas platelet count showed a protective effect (hazard ratio, 0.959; p<0.001). Negative binomial modeling demonstrated that higher weekly mean A-IPF was associated with fewer subsequent transfusions.
Conclusion:
A-IPF is a robust biomarker for early platelet engraftment and a clinically relevant predictor of platelet transfusion requirements in patients undergoing hematopoietic stem cell transplantation.
[…]