The journal einstein (São Paulo) – e-ISSN 2317-6385 is dedicated to dissemination of high-quality scientific content that advances our understanding of human disease with the goal of improving prevention, care, diagnostics and treatment of patients globally.
A 68-year-old man diagnosed with Chagas disease, hypertension and type 2 diabetes mellitus was followed up at a quarterly hospital in the specialties of otolaryngology and gastroenterology because of a chronic clinical feature of dysphagia and odynophagia for solid foods, and a non-confirmed diagnosis hypothesis of chagasic megaesophagus.
[…]
Forestier’s disease: a cause of dysphagia to recall
PereiraFOC, RomeroFR, Azevedo JuniorKC, LombardiIAS, RibeiroPW, GabarraRC, ZaniniMA. Forestier’s disease: a cause of dysphagia to recall. Einstein (Sao Paulo). 2014;12(3):380-1. https://doi.org/10.1590/S1679-45082014AI2659
Pereira,Francisco Otavio Camargo; Romero,Flavio Ramalho; Azevedo Junior,Kleber Carlos; Lombardi,Ismael Augusto Silva; Ribeiro,Priscila Watson; Gabarra,Roberto Colichio; Zanini,Marco Antonio. Forestier’s disease: a cause of dysphagia to recall. Einstein (Sao Paulo)., v. 12, n. 3, p. 380-381, Aug. 2014. https://doi.org/10.1590/S1679-45082014AI2659
Pereira,F.O.C., Romero,F.R., Azevedo Junior,K.C., Lombardi,I.A.S., Ribeiro,P.W., Gabarra,R.C., & Zanini,M.A. (2014). Forestier’s disease: a cause of dysphagia to recall. Einstein (Sao Paulo).,12(3), 380-381. https://doi.org/10.1590/S1679-45082014AI2659
Pereira,Francisco Otavio Camargo and Romero,Flavio Ramalho and Azevedo Junior,Kleber Carlos and Lombardi,Ismael Augusto Silva and Ribeiro,Priscila Watson and Gabarra,Roberto Colichio and Zanini,Marco Antonio. Forestier’s disease: a cause of dysphagia to recall. Einstein (Sao Paulo). [online]. 2014, vol. 12, n. 3, [cited 2026-02-20], pp.380-381. Available from: <https://journal.einstein.br/article/forestiers-disease-a-cause-of-dysphagia-to-recall/>. ISSN 1679-4508. https://doi.org/10.1590/S1679-45082014AI2659
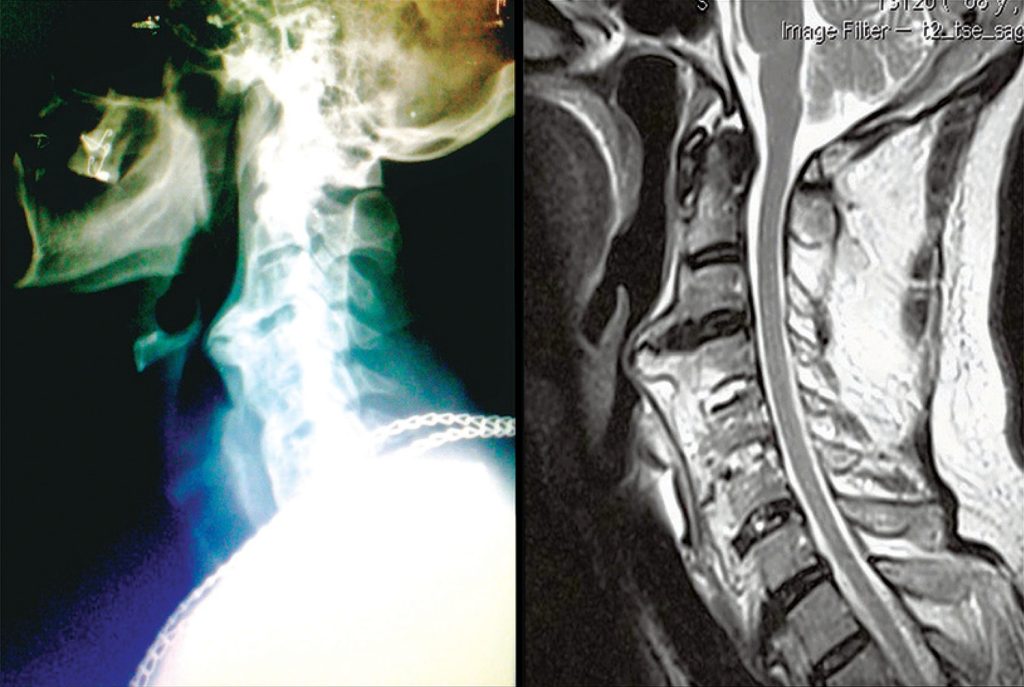
Lateral cervical X-ray and T2-weighted sagittal magnetic resonance. We observed an extensive calcification in front of vertebral bodies of C2 to C6 in topography of anterior longitudinal ligament. Esophagus and airways present a posterior compromising, which determine a stenosed segment that difficult orotracheal intubation at time of surgical procedure
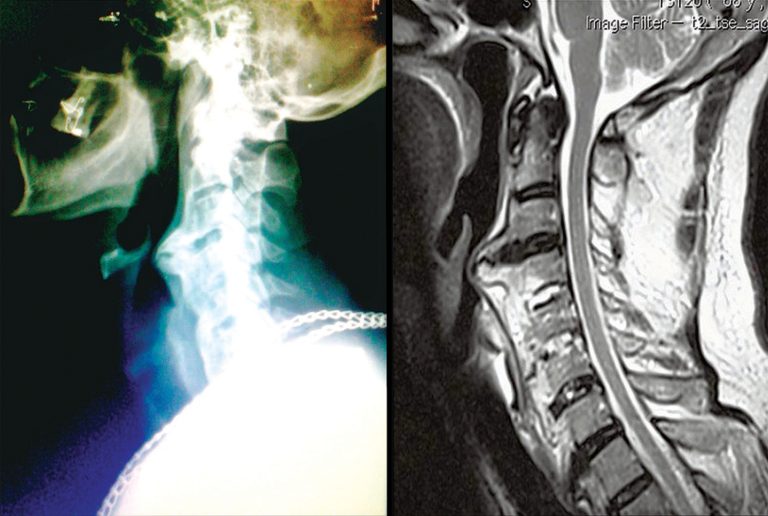
Lateral cervical X-ray and T2-weighted sagittal magnetic resonance. We observed an extensive calcification in front of vertebral bodies of C2 to C6 in topography of anterior longitudinal ligament. Esophagus and airways present a posterior compromising, which determine a stenosed segment that difficult orotracheal intubation at time of surgical procedure
Lateral cervical X-ray and T2-weighted sagittal magnetic resonance. We observed an extensive calcification in front of vertebral bodies of C2 to C6 in topography of anterior longitudinal ligament. Esophagus and airways present a posterior compromising, which determine a stenosed segment that difficult orotracheal intubation at time of surgical procedure
Lateral cervical X-ray and T2-weighted sagittal magnetic resonance. We observed an extensive calcification in front of vertebral bodies of C2 to C6 in topography of anterior longitudinal ligament. Esophagus and airways present a posterior compromising, which determine a stenosed segment that difficult orotracheal intubation at time of surgical procedure