einstein (São Paulo). 01/Oct/2011;9(4):550-1.
Congenital cytomegalovirus infection
DOI: 10.1590/S1679-45082011AI1687
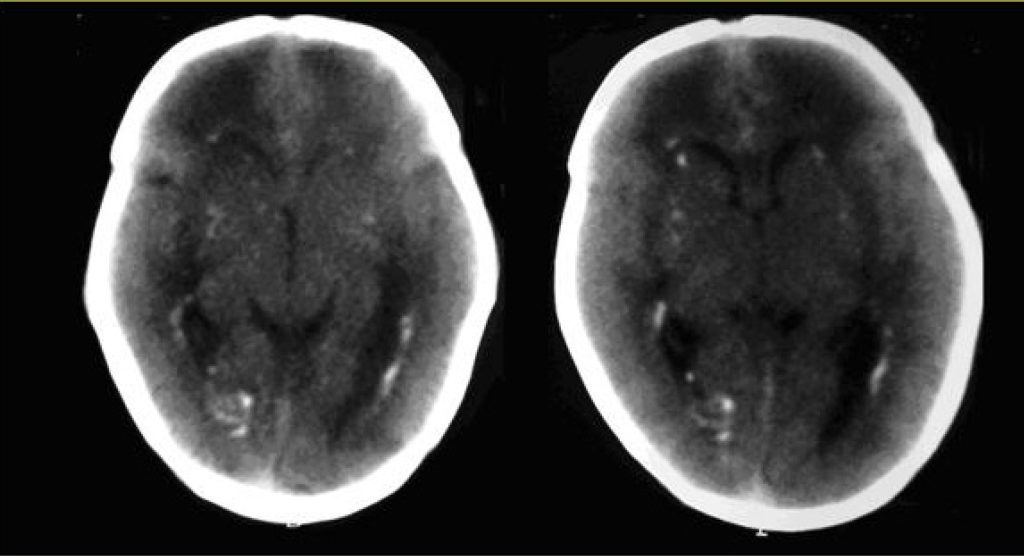
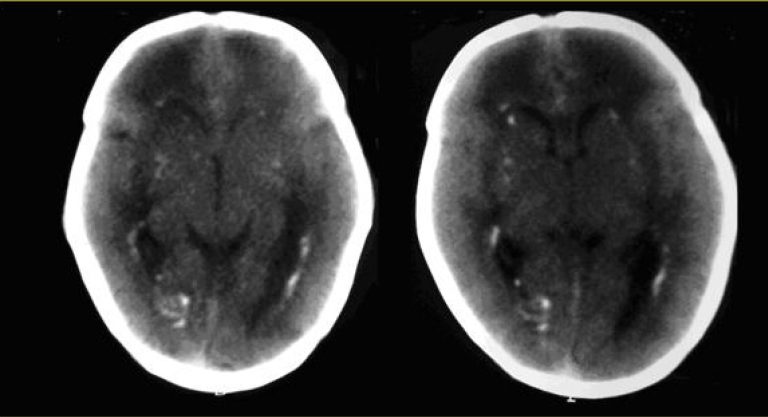
A female infant born at 37 weeks and 2 days of gestation by vaginal delivery was admitted to the neonatal intensive care unit on July 11, 2009 with birth weight of 2,030 g, height of 41,0 cm and head circumference of 31.0 cm. The infant Apgar were 8, 9 and 9 at 1, 5 and 10 min, respectively. A diagnosis of congenital toxoplasmosis was entertained because of the mother clinical history (she IgG positive and IgM positive for toxoplasmosis with avidity of 85% during first trimester of pregnancy). At the first trimester morphology scan intracranial calcifications were seen. The newborn had intrauterine growth restriction, splenomegaly, petechias and thrombocytopenia. Treatment of toxoplasmosis was done with sulphadiazine, pyrimethamine and folinic acid. The tomography of the skull showed multiple foci of bilateral periventricular calcifications and on the base nuclei. Due to these findings the serology for cytomegalovirus of mother and child was ordered. The mother was IgM negative, but IgG positive. The newborn was IgM and IgG positive. Cytomegalic inclusions in newborn’s urine and polymerase chain reaction (PCR) for CMV had positive results. The newborn was discharged and was referred to outpatient clinic to be treated with ganciclovir.
The congenital infections, syphilis, toxoplamosis, rubella, cytomegalovirus and herpes correspond to the acronym STORCH, and are characterized by common symptoms as: intrauterine growth restriction, hepatosplenomegaly, jaundice with increased direct bilirubin, anemia, petechiae, skin and mucosa lesions, encephalitis, pneumonia and thrombocytopenia(,). To diagnosis STORCH the most common methods are serological research of IgM and IgG, PCR and imaging exams. The clinical picture of toxoplamosis mainly shows hydrocephalus or microcephaly, diffuse cerebral calcifications in cerebral cortex, microphthalmia and chorioretinitis (due to microcephaly)(). The cytomegalovirus causes periventricular calcifications, and in ophthalmoscopy the chorioretinitis is not associated to microphthalmia. Herpes is identified when maternal genital herpes is diagnosed.
[…]
749