einstein (São Paulo). 13/fev/2026;24:eRC2117.
Difficulties in diagnosing a pediatric patient with small intestinal bacterial overgrowth
DOI: 10.31744/einstein_journal/2026RC2117
ABSTRACT
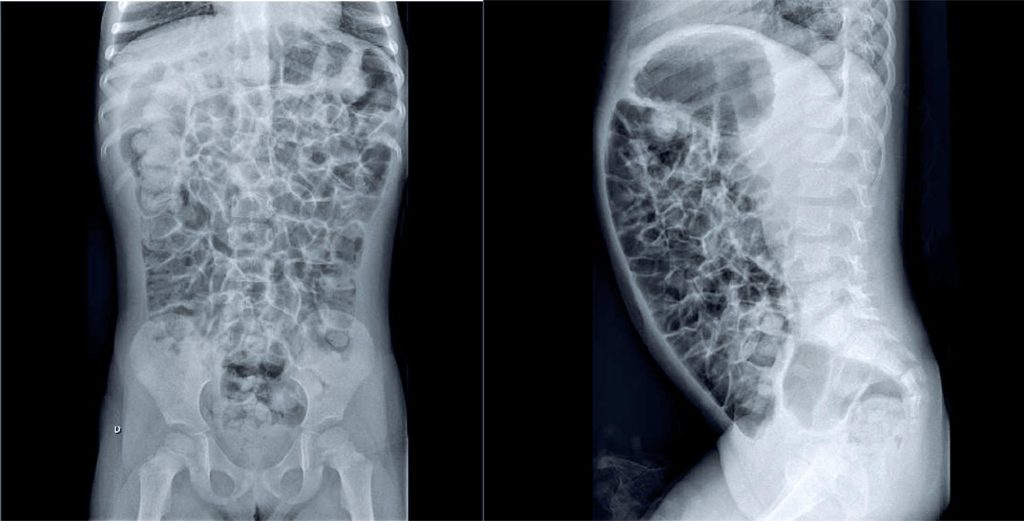
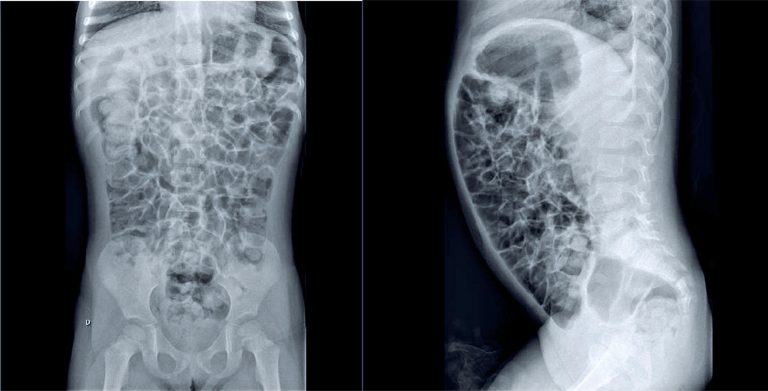
A 3.5-year-old female presented with a 10-month history of abdominal pain and distension, accompanied by frequent belching and flatulence. No nausea, vomiting, or nighttime awakening due to pain was reported, and the patient’s appetite remained intact. Growth and development were age-appropriate (weight: 16.2kg, height: 106cm). She was born at term without complications and had a normal neonatal screening. No comorbidities typically associated with small intestinal bacterial overgrowth (SIBO)—such as prior intensive care unit admission, immunodeficiency, food intolerance, Helicobacter pylori infection, anatomical abnormalities, prior abdominal surgeries, motility disorders, autoimmune conditions, or hepatic condition—were identified. Initial diagnostic hypotheses included more prevalent gastrointestinal disorders such as lactose intolerance, celiac disease, intestinal parasitosis, chronic constipation, and intestinal malformations (e.g., intestinal malrotation). SIBO was suspected following a thorough reassessment of the clinical history. The diagnosis was confirmed via a hydrogen breath test with lactulose, supported by radiological findings. Following treatment with metronidazole (30 mg/kg/day for 10 days), the patient demonstrated significant clinical resolution of the previously reported symptoms. A follow-up hydrogen breath test revealed no further evidence of bacterial overgrowth in the small intestine.
Palavras-chave: Gastrointestinal microbiome; Bacteria; Dysbiosis; Intestine, small; Child, preschool
9